Deputy sheriff Steve Singleton in an outing with the Rapid Response Team in Clermont County, Ohio - Danilo Verpa/Folhapress
Deputy sheriff Steve Singleton gets out of the car, puts on his hat, and knocks on the door of a ground floor apartment next to a bar in Clermont County, Ohio. It is an afternoon in February 2020, before the novel coronavirus pandemic. It is 0°C and raining, but the man who answers, a tall, burly blond, comes out to talk to him shirtless. Singleton does not put his hand on the gun at his waist; he does not try to search his home or announce an arrest; he doesn’t even enter the house.
In a calm voice, he introduces himself and asks if Kristy Mudd and Bryan Taylor, who are in the car, can come and talk to him. The man, who looks to be in his early 20s, had been arrested with meth a few days earlier; he had posted bail and awaited his sentence in freedom.
Kristy and Bryan had been drug users, and now they are part of the county’s peer counseling program, in which they play a role that combines the work of a sponsor in Narcotics Anonymous with that of a social worker. They stopped using drugs six and a half years and eight years ago, respectively, and today they are paid by the local government to help people seeking treatment for drug addiction.
Once a week, they go from house to house, following a list of people who have recently overdosed, been arrested with drugs, or whose families have asked for help. It’s called the Opioid Rapid Response Team. Even after the coronavirus arrived, the visits continued –everyone talks in a mask, without crowding, and outside.
“We have already been in your shoes, and we understand. We are proof that recovery is possible,” they repeat when starting conversations. Their mission is to convince citizens to seek treatment for dependence on illegal substances: most often, opioids –drug addict, heroin, fentanyl– or methamphetamine.
Nobody is forced to be treated, and they have no power to commit people involuntarily. The deputy goes along to help give the pair legitimacy and ensure their safety. However, according to the three, it is rare that they are greeted with violence.
The man in the apartment next to the bar denies abusing drugs and refuses treatment. Kristy and Bryan leave their cards with him –“you can call or text anytime,” she says– and a little bag with recovery brochures and Narcan, a nasal spray that reverses opioid overdoses.
The role of the Clermont Rapid Response Team shows how attitudes towards drugs are changing in the United States, starting with the focus of the police and the judicial system. If, during decades of war on crack, the country’s primary reaction has been to harden sentences and imprison, today in many places the policy of offering treatment to those arrested with drugs or committing crimes due to dependence prevails.
“Our priority is to protect life and property. This includes helping people not to destroy themselves,” says Steve Leahy, the county sheriff. “The truth is that the chains do not rehabilitate anyone.”
Ohio was one of the first American states to be overtaken by opioids and is one of the most affected by what later became an epidemic. Deaths from overdoses in the state rose from 2,110 in 2013 to 4,854 in 2017, the peak. In 2019, there were 3,957, or 34 deaths per 100,000 inhabitants, a rate comparable to that of violent lethality (intentional homicides, robberies, bodily injuries followed by death and deaths caused by the police) in the state of Rio de Janeiro.

Main street in Batavia, Clermont County, Ohio - Danilo Verpa/Folhapress
Clermont, about an hour’s drive from Cincinnati, the state’s third-largest city, has 200,000 people in rural or suburban areas. From 2009 to 2018, 700 died of an overdose. The local government began to modify its response to the crisis in 2013, with the creation of the Opioid Task Force. Since the peak of 105 deaths in 2015, the number has been falling.
The opioid epidemic has burdened counties financially. The costs range from rescuing and treating dependents to sheltering children separated from their parents by death or hospitalization and paying coroners for autopsies of overdose deaths.
Two features of the opioid crisis explain why the United States began to change its outlook on drugs with the epidemic. The first is that the abuse was distributed in an unprecedented way, geographically and socially: it started in rural areas, but then it also reached suburbs and large cities, dragging people of different profiles and social classes. The image of drug abuse was not limited to a single group, as was the case with crack cocaine in the 1980s and 1990s, which was seen as a problem for blacks in degraded urban areas.
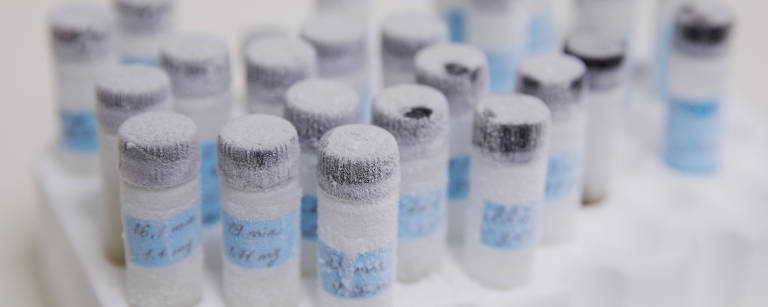
The second characteristic is the lethality of opioids when compared to other drugs. One of the main tools to prevent deaths is naloxone or Narcan. Now available as a nasal spray, the drug reverses the effects of opioid overdoses, in which the drug causes depression of the central nervous system, and the user stops breathing. Naloxone, which is not addictive, temporarily “removes” opioids from brain receptors, allowing the person to breathe again.
“Narcan changed the game,” says Sheriff Leahy, who, like others heard by Folha, sees the drug as one of the main factors responsible for the drop in the number of deaths from opioid overdoses. The sheriff’s officers carry the medicine with them at all times.
Another important change is that treatment with the aid of medicines (known by the acronym MAT, medically-assisted treatment) has become the standard for the recovery of addicts. Methadone has been prescribed for decades to help control cravings for heroin and other opioids. Now there is also buprenorphine and naltrexone, which help control the symptoms of withdrawal.
“When we started offering MAT, around 2009, we called the state department of mental health and drugs, and they said they didn’t support this type of treatment,” says Karen Scherra, executive director of the mental health and recovery council for Clermont county. Today, MAT is public policy in Ohio.

The Community Alternative Sentencing Center in Clermont County, Ohio - Danilo Verpa/Folhapress
Anyone arriving at the Maryhaven treatment center in Columbus, the state capital, is greeted by a police officer. But even if the person arrives with drugs or an open warrant, he will not be arrested.
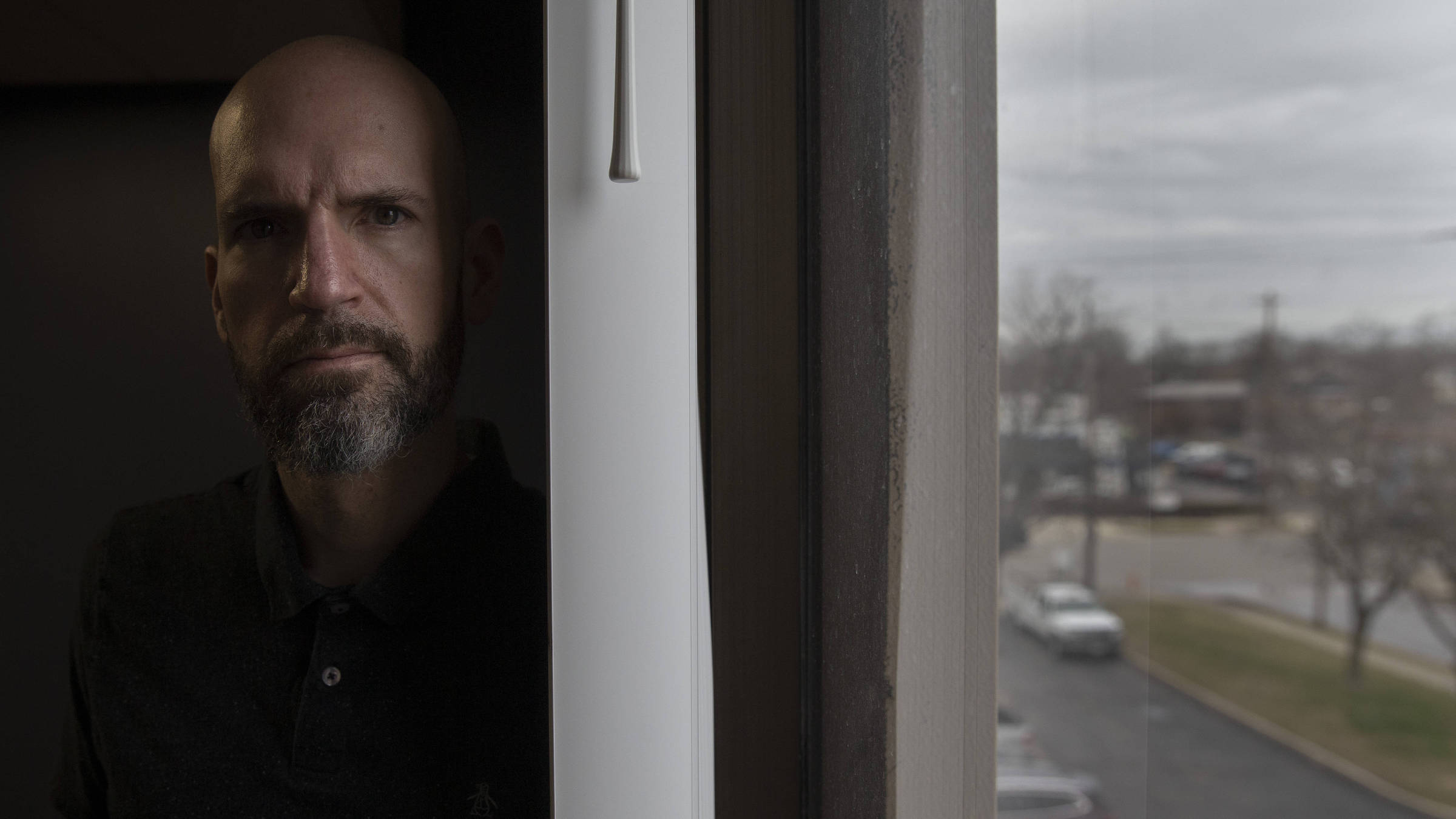
Nate Blake, 42, went through treatment at Maryhaven five times; since the last time, ten years ago, he has been without drugs. “Some people think that going into treatment will fix you, but it’s just the beginning of a process lasting years. It took me a while to understand that I was born with a drug addiction disease and that I could never use any substance again.” He started using drugs –several, including opioids– at the age of 19. “I decided to stop using heroin when my best friend died of an overdose in my arms. Then I thought: I’m just going to drink and use crack like a normal person.”
When he was last admitted the last time, he used drugs for alcohol withdrawal. He spent seven weeks in residential treatment and then months in a home for people in recovery. But getting his life on track took much longer.
Nate Blake, a recoveiro addict who works at Maryhaven treatment center in Columbus - Danilo Verpa/Folhapress
“I had never been a real adult. When I stopped using drugs, I only did little temporary jobs, because I was sure that if I got a job, it would go wrong. Only after four or five years sober I realized that I could work a full-time job”, he says.
“Everything scared me, the prospect of going on a romantic date or a job interview sober was terrifying,” says Nate. “There are few who can do it all on their own.”
Today he uses his experience to help others: he works as a counselor at Maryhaven, conducting group meetings, and accompanying patients to court dates, helping them to solve bureaucratic problems and navigate life.
The so-called Dependency Stabilization Center is always open to receive people who want to be treated immediately. On the ground floor, patients are stabilized, usually within 12 hours. Then they go up to the third floor, where the abstinence management section is located. The vast majority opt for MAT: take medication and participats in therapies (group and individual), support groups, and other activities.
“When you stop using it, there is a flood of memories, guilt, and shame that can be more difficult to deal with than physical symptoms [pain, nausea, and sweating, among others],” says Daniel King, Maryhaven’s administrative coordinator.
In one wing there are men and in another, women. At the ends of each corridor there are chairs and a TV on which, between activities, patients watched soap operas on the day of the Folha’s visit, a Tuesday afternoon. The atmosphere is not cheerful, but it is quiet; the staff is kind and empathetic. Walls are decorated by the patients with motivational designs and phrases.
Phrases written by patients at Maryhaven, in Columbus - Danilo Verpa/Folhapress
After this phase, patients go to residential treatment in another building, where they can stay for up to 21 days. During recovery, many people need several services to which Maryhaven refers them: treatment for other health problems; help obtaining health insurance, benefits, employment or housing; assistance with judicial disputes; and family services, for those who have lost custody of their children, for example.
“In the first few weeks of abstinence, we have to manage the patient’s physical needs. This is the part that users are most afraid of. But in the following weeks, it is often even more difficult, because the bills come due, literally and metaphorically. Debt, court hearings, problems at work, family issues –the stress is enormous,” says doctor Mike Kalfas.
He has worked with drug users for 23 years in northern Kentucky, near the Ohio border, a region also hard hit by opioids. According to him, it is in this second moment of recovery that many relapse.
The trajectory of someone who tries to stop using drugs is not usually limited to a single hospitalization followed by success. Some continue to take the medication for months or years; others check-in repeatedly.
Kalfas compares the addition to a chronic illness, such as diabetes, which must be managed for the rest of the patient’s life.
Sam Sherbourne, 29, is at the beginning of this recovery journey. She had been using meth and fentanyl for about two years when, pregnant, she was arrested.
“My biggest fear was having the baby in prison because the Department of Children’s Services would get involved [and could take custody of the child],” she says. The judge referred her for treatment at First Step Home in Cincinnati, instead of sentencing her to prison. “I was ready to be helped. It was a relief,” she says.
First Step Home is a women’s-only residential treatment center that occupies a block in a quiet neighborhood. There, patients can stay with their young children while they recover.
Sam gave birth to Maleah in a hospital within days of arriving and is now in the First Step postpartum ward. She takes buprenorphine and participates in individual and group therapies. Maleah, who was two months old at the time of Folha’s visit, undergoes weekly consultations, because she was born with health problems resulting from the use of drugs during pregnancy.

Sam Sherbourne and her daughter Maleah at First Step Home, in Cincinnati] - Danilo Verpa/Folhapress
Sam’s story illustrates another major change in public policy: at the beginning of the epidemic, thousands of children were separated from their drug-dependent parents. Today it is more frequent to offer treatment and social assistance while trying to keep the family together. Even in the case of pregnant women, it is becoming more acceptable to keep mother and baby together, if possible and safe for the child.
Overdose deaths in the US, after falling in 2018, rose 4.6%, to almost 71,000 in 2019. Among the explanations is the spread of fentanyl, more potent, and methamphetamine, for which there is no MAT or medicine that reverses overdoses.
The arrival of the coronavirus threatens advances: fewer people are showing up for treatment for fear of Covid-19. Social isolation, boredom, unemployment –about 30 million in the country had lost their jobs by the end of July– and the lack of face-to-face meetings of Alcoholics Anonymous and Narcotics Anonymous are leading to relapses, according to doctors and social workers.
Using opioids alone at home is also more dangerous, as there is no one to call for help or administer Narcan in case of an overdose. There is no consolidated data yet, but Ohio experts have noticed more overdose deaths since the pandemic began.


Night view of Cincinnati, Ohio - Danilo Verpa/Folhapress